

Introduction
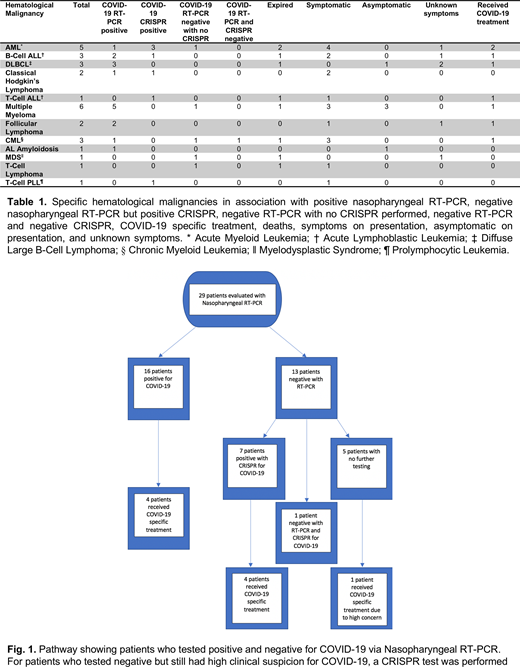
Patients with hematological malignancies (HM) are uniquely immunocompromised and considered at high risk for COVID-19. However, data regarding the diagnosis, clinical course, treatment, and outcomes of these patients is sparse. In particular, the ability to successfully detect SARS-CoV-2 in patients with HM remains unknown. We have previously reported 2 cases of allogeneic stem cell transplant (SCT) diagnosed with COVID-19 using clustered regularly interspaced short palindromic repeats (CRISPR) technique, following multiple negative nasopharyngeal RT-PCR testing (Niu et al. Bone Marrow Transplantation - Nature). Here we examine 29 patients with a variety of HM with high suspicion for COVID-19 based on clinical presentation, lab results, and imaging, whom were tested with CRISPR and/or RT-PCR based techniques. From 3/31/20 to 7/17/20, 29 patients (age 24 to 82) with a variety of HM (20 lymphoid, 9 myeloid; Table 1), 24 of which presented with an undiagnosed respiratory illness and 5 presented while asymptomatic for testing prior to chemotherapy, were evaluated for COVID-19. While 16 patients tested positive for COVID-19 with guideline-directed nasopharyngeal RT-PCR testing (including the 5 asymptomatic patients), 13 patients tested negative with the same technique. However, based on their clinical history, imaging, and disease course, concern for COVID-19 infection remained in these 13 patients. We then used CRISPR technology available at our institution (Huang et al. Biosensors and Bioelectronics) to test 8 patients who initially tested negative by RT-PCR. Surprisingly, 7 of the 8 patients tested positive for COVID-19 with either a blood sample and/or nasal swab for the SARS-CoV-2 specific N gene and ORF1ab gene. Excluding the patients who were negative by RT-PCR and not tested by CRISPR, the rate of false negativity with RT-PCR testing is significantly elevated at 29% (7/24) in our cohort of HM, which compares unfavorably with the expected false negative rates of RT-PCR techniques.
A very high fatality rate was observed with 9 out of the 29 patients (31%) ultimately dying. Fifteen patients were undergoing active chemotherapy, 4 had received an autologous SCT, 6 had received an allogeneic SCT, and 4 were on surveillance. Of the 23 COVID-19 positive patients (by RT-PCR or CRISPR), 8 patients received COVID-19-directed therapy with either hydroxychloroquine/azithromycin, remdesivir, and/or Covid-19 convalescent plasma (CCP) depending on their clinical status, and 4 patients expired. Of the 8 treated patients, 7 improved while 1 patient expired. For the 5 patients who were negative for RT-PCR with no CRISPR completed, 1 patient received hydroxychloroquine/azithromycin proactively due to symptoms and imaging and recovered, while 3 patients expired at outside facilities due to unknown causes. Breakdown of testing and treatment is shown in Fig. 1.
The majority of our patients had undergone SCT or were actively on chemotherapy, notably lymphodepleting chemotherapy. Associated with the fact that COVID-19 is known to worsen lymphopenia, our patient's symptoms and immune response to COVID-19 is likely to differ from immunocompetent hosts. This translated into an overall worse outcome as seen by the high mortality with our patients. In our limited dataset, patients presented with a variety of symptoms ranging from asymptomatic to acute respiratory failure. Intriguingly, the 5 asymptomatic patients had lymphoid malignancies and were on chemotherapy.
It is thus imperative to establish the diagnosis of COVID-19 quickly, as faster initiation of treatment has been associated with better outcomes. The 8 patients who were diagnosed and treated improved substantially. However, as seen by our dataset, a strikingly high false negative rate was observed. Thus, a high clinical suspicion must guide further workup and therapy in patients with HM who present with an undiagnosed respiratory illness consistent with COVID-19. Patients with HM can have a wide variety of presentations when infected with COVID-19. For this select patient population we must establish an algorithm to diagnose COVID-19 efficiently as we reported a high number of initial false negative COVID-19 tests before the more sensitive CRISPR revealed a positive test. In addition, treatment pathways need to be instituted to not only treat COVID-19 infection, but also provide the best treatment for these patient's underlying HM.
Safah:Amgen: Honoraria; Verastem: Honoraria; Janssen: Speakers Bureau; Astellas: Speakers Bureau. Saba:Kite: Other: Advisory Board; Pharmacyclics: Other: Advisory Board, Speakers Bureau; AbbVie: Consultancy, Other: Advisory Board, Speakers Bureau; Janssen: Other: Advisory Board, Speakers Bureau; Kyowa Kirin: Other: Advisory Board.

